Language development disorder
What is a Language Development Disorder?
A language development disorder, also called TOS, is a neurobiological developmental disorder. As a result, language is less well processed in the brain. Children with TOS have difficulty speaking and do not understand language well. As a result, their speech and language development is different from that of children of the same age. Children with a developmental language disorder can hear well and have normal intelligence. They have difficulty learning language and find it difficult to remember sounds and words. They also have problems with grammar. In addition, they find it difficult to deal with emotions, just like making a plan.
Signs that may indicate a language development disorder
TOS may be present if the child:
• speaks in short, illogical sentences• is poorly understood• is quiet and talks little • has difficulty concentrating• often does not understand others• sometimes does not seem to listen
What do I do as a speech therapist with language development disorder?
Language problems can be caused by TOS. In addition, there are other causes. I will therefore often propose an overall developmental examination that can be taken at an audiological center. This overall developmental examination consists of a psychological examination, speech therapy examination and a hearing examination. This makes it possible to determine whether the language problems are indeed the result of a language development delay. Other causes of language problems include general developmental delay, speech development delay, hearing problem, auditory processing problem, or information processing problem.
What are the consequences of language development delay?
Language development has a major impact on a child's daily life. This becomes visible in, for example, learning and reading problems, maintaining friendships and behavioral problems. Some children with TOS become silent and withdrawn, others react aggressively. A TOS can have a major impact on both the child and the parents.
The difference between a language development disorder and a language delay
A language development disorder is different from a language delay. A language delay occurs when a child hears or speaks little of his mother tongue. This backlog can be made up again later. A language development disorder has to do with the innate ability for language skills. That is why specialist treatment is required. TOS is a predisposition disorder. That is why a child will always suffer from it to a greater or lesser extent.
Multilingualism
We speak of multilingualism when children come into contact with two or more languages during their development. For example, parents with different mother tongues or children of non-native parents who are offered a different language at home than at school.
Speech development disorder
A speech development disorder is present when the child's speech clearly lags behind that of peers.
Young children usually pronounce the words incompletely. For example, 'toe' for 'chair' or 'ba' for 'ball'. Some children continue to make pronunciation errors longer than usual. This can affect intelligibility to such an extent that the child is sometimes unable to make himself/herself clear. A child of five years can pronounce most sounds well.
A delay in speech development causes problems: the child is not understood by the environment and cannot express himself well. This can lead to behavioral problems: the child becomes rebellious and hot-tempered if it is not understood or it starts to withdraw more and more. Learning at school can also be more difficult.
What do I do as a speech therapist with delayed speech development?
A speech test is performed on the child. Among other things, standardized tests are used. Speech therapy treatment is indirect and/or direct. In indirect therapy I explain to the parents how they can stimulate the child to speak. In direct speech therapy, the interaction between child and me is central. The outcome of the treatment depends, among other things, on the cause of the delayed development. In general, delayed speech development can be treated well, especially if the problems are recognized at an early age. Children can already go to speech therapy before their second year of life.
Voice problems
Vocal problems can also develop early on in children. This can have various causes, for example by talking too much, too long and/or too loud in class or in the schoolyard or by making crazy voice sounds too often. Doing this a lot creates a lot of tension in the muscles needed for talking. If this goes on long enough, it can even damage the vocal cords and lead to vocal cord nodules. Sometimes a voice can suddenly be completely gone and all you can do is whisper.
When do voice problems arise?
- Hoarseness (longer than 2 weeks)
- Hoarse voice Crackling voice
- Too high or too low a speaking voice
- Pain in the throat when or after speaking
- Having a painful, burning sensation in the throat after speaking
- Loss of voice No longer being able to shout or sing
- Constantly having to clear the throat
- Voice drop or rise (in puberty) Insufficient recovery after a cold: when complaints persist for more than 4-6 weeks
- Hoarseness or throat complaints due to incorrect use of the voice
- Hoarseness or loss of voice after illness or surgery
- Vocal cord nodules identified by the ENT specialist
Stuttering
The development of stuttering and the factors that trigger it can be different. Most young children have a phase when speaking is not fluent, but some children continue to speak stuttering for longer. Some become mild to severe stutterers.
What do I do as a speech therapist with stuttering?
During the research, we listen to which stutters are made, how often they occur and the tension they evoke. On the basis of a questionnaire I look at how your child perceives his own seriousness of stuttering in different situations and whether this happens with a feeling of satisfaction. All answers from the study are included in the treatment plan to tackle stuttering as completely as possible. Depending on the severity of the stuttering, I work on 'talking without stuttering', so speaking as fluently as possible is practiced with the child with appropriate techniques. Sometimes the therapy is limited to a consultation with you as a parent, in which it is indicated how you can stimulate your child to speak fluently, ie without stuttering.
If your child has been stuttering for some time, it may be that more attention is needed for your child's self-image. How does your child feel about the speech problem and does he or she want to consciously change this? The therapy continuously monitors your child's development.
Abnormal oral habits/OMFT
We speak of abnormal oral habits if the habitual actions or movements are negative for the position of the teeth, speech, hearing and health. You can think of, for example, abnormal swallowing and chewing and habitual mouth breathing. Incorrect lip and tongue habits are also part of deviant oral habits.
What is abnormal swallowing behaviour?
Abnormal swallowing means that someone swallows with the tongue low in the mouth. Sometimes this swallowing behavior is caused by mouth breathing, but that is not always the case. During swallowing, the tongue pushes hard against the teeth, which can cause them to become crooked. When speaking, the tongue can also get between the teeth, causing slurred speech.
When is abnormal swallowing behavior treated?
Abnormal swallowing behavior in children is treated before or after changing the front teeth and often from the age of 7 years. It is not possible to train properly during the switch. You really need the front teeth for that. I look at what is best for your child and will tailor the treatment accordingly.
What are the consequences of abnormal swallowing behaviour?
The shape of the mouth and the position of the teeth are largely determined by the function of the tongue and the muscles in and around the mouth. If the tongue is in the wrong position at rest and during swallowing, you often see this also during articulation. Especially during the pronunciation of /t/, /d/, /n/ /l/, /s/ and /z/ there is often a wrong tongue position against or even between the teeth. The so-called hissing or lisping.
What is habitual mouth breathing?
Habitual mouth breathing means that you do not breathe through the nose, but through the mouth. The lips are not closed even at rest. Habitual mouth breathing often occurs when you have breathed through your mouth for a while because of a narrowing in the nose. This is usually related to an allergy or cold. Once the nose is open again, the habit of breathing through the mouth is so ingrained that it persists.
What are the consequences of mouth breathing?
When breathing through the nose is almost stopped, the mouth muscles become weaker. In addition, the mouth becomes drier and swallowing is less frequent. When swallowing, the Eustachian tube is opened. That is the connection between the nose and the ear. If this tube opens too little, there is a greater chance of ear infections and other health problems.
What do I do as a speech therapist in case of abnormal oral behaviour?
If young children have mouth breathing, it is important to treat this problem in time. I mainly focus on closing the lips and strengthening the mouth muscles. Targeted exercises also train the muscles of the lips and tongue.
OMFT
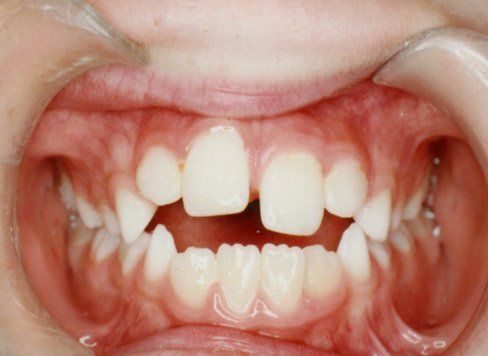
Oromyofunctional therapy is an exercise therapy aimed at restoring the balance in the functioning of the muscles in the mouth area. By unlearning bad habits/reflexes and balancing the muscles of the mouth, the position of the jaws and teeth is improved. The shape and function of jaws and teeth can be restored. The abbreviation for this is OMFT.
Function affects form. A wrong function of the muscles has a negative influence on the form. If the cause is removed, orthodontics has a high chance of success, and the chance of a relapse is smaller.
Below you can see the effect of OMFT



Reading and spelling difficulties
The first signs of reading and spelling difficulties can be visible early on, for example in group 2 when preparing for learning to read and spell. There may be problems in letter knowledge, phonemic awareness (distinguishing sounds in a word) or automation. In group 3 or the higher groups of primary education it is often noticeable that the sound-sign coupling and the application of the spelling rules cause difficulties. While reading, children may have difficulty with reading pace or reading accurately. This can cause problems in reading comprehension.
What are the consequences of reading and spelling difficulties?
When there are problems with (learning) reading and/or spelling, this can lead to a reading/spelling delay. This can ensure that a person with reading difficulties does not become sufficiently skilled in reading and/or spelling and therefore cannot cope sufficiently at school, during work and in other areas of daily life. When reading smoothly and accurately and/or spelling correctly is not successful or difficult, this can lead to insecurity, shame, reduced self-confidence, etc. It is therefore important to call in early guidance.
What do I do as a speech therapist with reading and spelling difficulties?
Advance training can be given to younger children with difficulties in the initial reading and spelling development. Later on, a systematically structured training is offered in which spelling rules for the written language are discussed. Furthermore, reading motivation and fun are central. To reduce the influence of reading and spelling difficulties on school functioning, speech therapy can practice the use of compensatory techniques such as text-to-speech software and mind maps.
I am not authorized to issue a dyslexia statement, but I can give advice on further diagnostics. In addition, I can demonstrate persistence through extra guidance.